Night shifts for me have tended to present opportunities to disappear into various creative rabbit holes and contemplate areas to optimise. Maybe it’s inherent in the increased level of stress caused by this upside-down schedule, rendering my mind a minefield of thoughts whizzing around like excitable electrons.
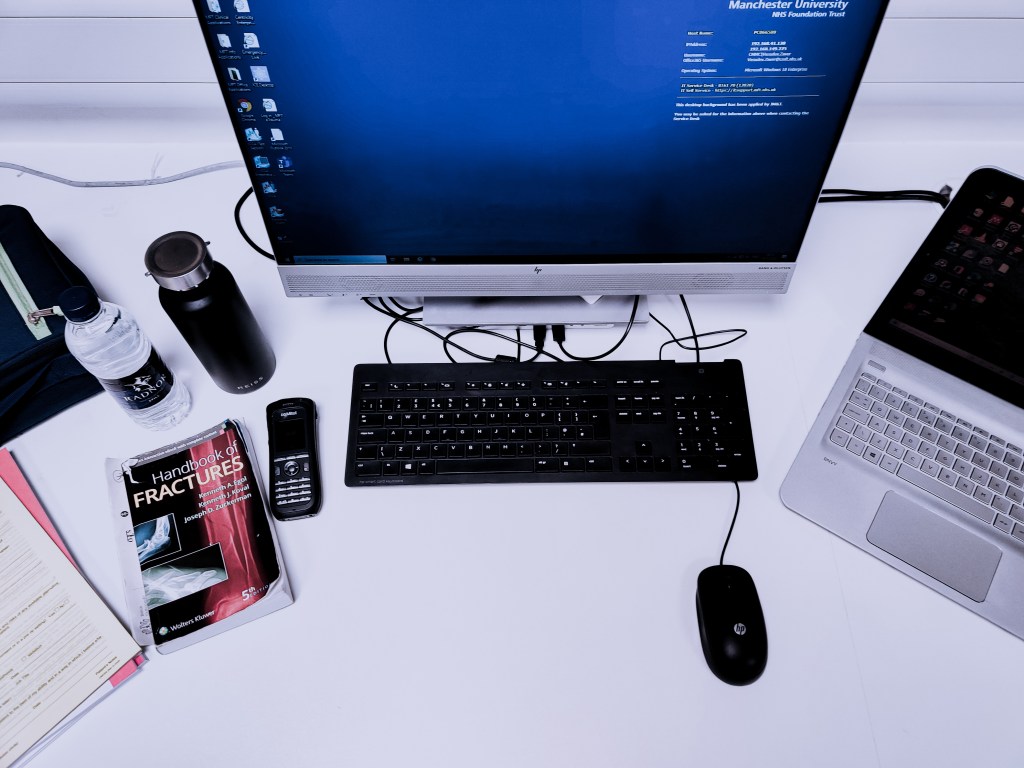
Through serial iterations of the optimal kit list to take into the hospital for night shifts, I thought I’d share the items that have made it onto my own shortlist. In Trauma & Orthopaedics at senior house officer (SHO) level (which can be anywhere from Foundation Year 2 (FY2) level to Core Surgical Trainee), the night shift is usually a lonely affair. In most hospitals across the country, the registrar is non-resident, which means they are away from the hospital site at home or asleep in nearby accommodation. Unless you really need to call for backup, it’s all a solo run.
That’s why I like to make sure I’m well kitted out. As I’ve alluded to in previous career talks, a Trauma & Orthopaedic on-call shift essentially comprises orthopaedics, medicine, and anaesthetics; it’s crucial to have an awareness of all three of these domains in order to perform the job to a high standard. Obviously, the escalation protocol is there if senior or other specialty input is required, but the key aspect is the ability to recognise problems that could impact a patient’s life or limb-saving surgery.
The key aspect is the ability to recognise problems that could impact a patient’s life or limb-saving surgery
- Accordingly, it is only fair to kickstart the list with a stethoscope as the first item. Whilst this is ostensibly an unorthodox piece of apparatus for a surgical doctor to carry, I strongly feel it’s important to have the bare necessities to perform a fundamental systems examination on a patient. How else would I be able to tell the anaesthetist about the ejection systolic murmur in the patient with a neck of femur fracture at the morning trauma meeting otherwise? Or if a patient deteriorates, I need something aside from my mythical surgical x-ray vision to perform a suitable workup in order to convey a decent history to the medical team when escalating. So, a stethoscope very much resides on my person.

- The next item in the toolkit is a pair of robust scissors. I always find that scissors that are strong enough to cut through thick plaster sodden crepe bandage and wool are nigh on impossible to find. More often than not, a well-intentioned healthcare staff member will bring the smallest scissors known to mankind, in complete earnest, but totally missing the mark as regards function. The only way to master this predicament is to purchase a pair of thick scissors with a slight serration on one of the blades, usually referred to as “Tuff Cuts”. It’s a game-changer and evokes a moment of true wonderment in the Accident and Emergency department that an orthopod has their own kit on them.

- The third addition to my motley arsenal is a set of three pens. Well, strictly speaking, not all three items are pens. One is a pen torch. But I’m feeling generous so I have permitted it to join its oblong comrades. Nonetheless, all three cylindrical objects are on my person 100% of the time. A pen torch is incredibly handy when looking at wounds at night under the single lumen lighting that features on most hospital wards. Or to examine pupils, but naturally this is less often. Marker pens are for marking the surgical site in patients who are due to undergo surgery. Those who are particularly astute may wonder why on Earth I need two permanent marker pens. The short answer: I’m greedy, it’s complicated, and it has something to do with hospital politics. Just trust me…
A pen torch is incredibly handy when looking at wounds at night under the single lumen lighting that features on most hospital wards.

- The fourth and final item in my kit list is a fat handbook of fractures. Generously gifted to me by a good friend, it has gone from well thumbed to even more thoroughly thumbed since finding itself in my possession. It’s taken me several months of orthopaedic on-call shifts to acknowledge the learning opportunities offered by this aspect of the job. The consolidation of on-the-job exposure through extra reading has been a powerful tool for me to rapidly improve my knowledge and capabilities during clinical rotations. Say what you will about supervised learning events such as case based discussions (CBDs)), but these portfolio-based activities provide immeasurable utility as a way to document newly learned information.
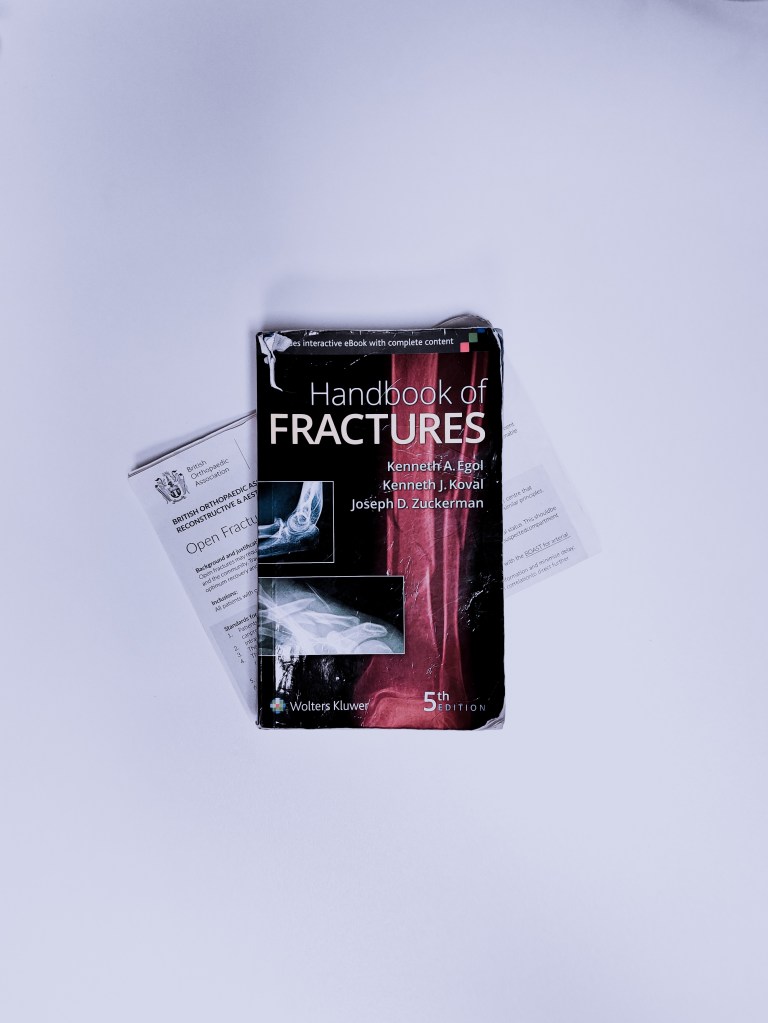
The consolidation of on-the-job exposure through extra reading has been a powerful tool for me to rapidly improve my knowledge and capabilities during clinical rotations.
In general, I also like to have my laptop with me to complete my own work if I have any time to myself during night shifts. I’m not one to sleep as it disrupts my sleeping pattern during the day, and besides, I enjoy the spare time to catch up with outstanding administration or assignments. Lastly, a good and ample packed lunch is essential. The last thing I want to be during nights, on top of raised baseline cortisol, is “hangry”. That’s akin to a grammatical travesty I once read on social media: “I would rather be pissed off then pissed on” (it’s supposed to read “*than pissed on”, in case it wasn’t clear).
